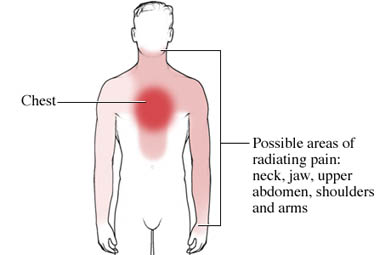
Prinzmetal’s angina is a form of chest pain, pressure, or tightness (angina) caused by spasms in the arteries that supply blood to the heart.
It is a form of unstable angina, meaning that it occurs at rest, often without a predictable pattern. This is in contrast to stable angina, in which chest pain occurs in a predictable pattern during exertion or exercise.
Episodes of chest pain caused by Prinzmetal’s angina usually occur in clusters, with periods of frequent episodes lasting for a few months followed by weeks or months with no chest pain episodes. The pain usually occurs between midnight and approximately 8:00 AM. Prinzmetal’s angina may be brought on by hyperventilation, exposure to cold, or extreme emotional stress.
Prinzmetal’sangina is named after the researcher who first noted that coronary artery spasms were to blame. It is also called variant angina because of the unusual pattern of chest pain episodes.
The chest pain of Prinzmetal’sangina is caused by coronary artery spasm, an abnormal or involuntary constriction of the muscle in a coronary artery. This spasm makes the diameter of the artery smaller, restricting the supply of blood and oxygen to the heart, causing chest pain. In rare cases if the spasm is not
Prinzmetal’sangina is relatively rare and the actual number of cases is not well documented. About 4 out of every 100,000 Americans have it, or about 2% to 3% of people with chest pain who undergo an X-ray of the heart called a cardiac catheterization (also known as an angiogram). Men are more likely to suffer Prinzmetal’sangina than women. It also seems to be more common among Japanese people than Caucasians. People with Prinzmetal’sangina are generally younger than those with stable angina; the average Prinzmetal’s angina patient is between 51 and 57 years old. They also have fewer risk factors for heart disease with the exception of smoking, which is the most significant risk factor for coronary artery spasm.
The majority of people with Prinzmetal’sangina also have coronary artery disease, characterized by atherosclerosis. Prinzmetal’s angina alone rarely causes a heart attack, but heart attacks may occur more often in patients with severe underlying heart disease. There is also a very slight risk of sudden death (about 2%) in people with Prinzmetal’s angina.Coronary artery spasms can also be silent, meaning they occur without any symptoms.
Symptoms of Prinzmetal’s angina:
- Located under the chest bone
- Described as squeezing, constricting, tightness, pressure, or crushing, which is usually severe and may radiate to the neck, jaw, shoulder, or arm
- Often occurs at rest
- May occur at the same time each day, usually between 12:00 midnight and 8:00 AM
- Lasts from 5 to 30 minutes
- Relieved by nitroglycerin
- Can cause fainting or loss of consciousness
What causes coronary spasms?
It is not known exactly what causes coronary spasms. They may be due to problems with the thin lining of the blood vessels called the endothelium. Usually the artery lining produces a chemical (nitric oxide) that widens the blood vessel allowing blood to flow through with ease. If the artery lining is damaged or isn’t working properly, the blood vessels may narrow more easily, which may cause a coronary spasm. This idea is supported by research done in women. Levels of the artery-widening chemical are higher when estrogen levels are also high at certain stages of the menstrual cycle. Studies have shown that during these times when estrogen levels are high, women have fewer chest pain attacks. Smokers tend to have lower levels of nitric oxide in their blood vessels than non-smokers, and smoking is a major risk factor for coronary spasm.
However, there is also research suggesting that the nitric oxide theory doesn’t fully explain Prinzmetal’s angina. Atherosclerosis, the hardening of the arteries caused by the buildup of fatty plaque, impairs the release of nitric oxide, but not everyone with atherosclerosis develops coronary artery spasms.
Prinzmetal’sangina is often diagnosed with an ECG (electrocardiogram or EKG) during an episode of chest pain. The ECG may show a particular pattern called ST segment elevation:

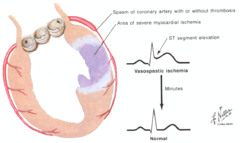
The pattern will disappear when the chest pain resolves. If you do not have heart disease (meaning an X-ray of your heart shows no major blockages in the arteries of your heart) or have only mild heart disease, and this pattern appears during ECG testing, you will probably be diagnosed with a Prinzmetal’sangina.
Prinzmetal’sangina is treated with medications, specifically nitroglycerin (NTG), long-acting nitrates, and calcium channel blockers, all of which widen or open the blood vessels and improve blood and oxygen flow to the heart muscle. Calcium channel blockers are generally prescribed first. If you continue to experience episodes of chest pain, then a different class of calcium channel blocker or a long-acting nitrate may be given.
Nitroglycerin is used when you are experiencing a spasm to stop it, thereby alleviating pain; it is not used as a preventive medication. Nitroglycerin is usually given as a spray that you use in your mouth or a tablet that you place under your tongue.
Risk factor modification is also important because most people with Prinzmetal’sangina also have heart disease and are therefore at risk for a heart attack. It is especially important to stop smoking because smoking increases the likelihood of coronary artery spasms.5 By lowering your risk factors, you will reduce your chances of developing atherosclerosis. In addition, people diagnosed with Prinzmetal’s angina should avoid exposure to cold and high stress situations since these can trigger spasms.
What is the prognosis for people with Prinzmetal’sangina?
With medication, the prognosis is very good for people with Prinzmetal’sangina, and their chest pain can be treated successfully.
Prognosis is closely tied to the extent of coronary artery disease, and people with more severe heart disease have worse outcomes than those with less severe or no heart disease.The severity of the spasm, and how completely it blocks blood flow to the heart, may also predict outcomes: in one study, people who had ST-elevation on an ECG were 3 times as likely to die or have a heart attack than those who did not, independent of the extent of their coronary artery disease.Variant angina also increases the risk of developing a cardiac arrhythmia, and there is a small but significant risk of sudden cardiac death. Sudden cardiac death occurs most often in people who have spasm in multiple arteries and have experienced an arrhythmia before during a chest pain attack.
Comments 4
Thank a very helpful artical
You didn’t mention a connection with Reynaud’s which was noted in my case. Cold, vibration and emotional stress are the stressors that bring mine on. Dressing to block cold [layered and with either ski mask or using a muffler to breath through is very effective for me. I also avoid riding on riding mowers, go carts where the vibration comes up my legs and arms are the second most frequent cause. Only once did it come from stress [I had a very low blood sugar [T1D], a full bladder and a hysterical boss yelling at me that I “was just making excuses and would NOT be allowed to leave the demo area to use the bathroom.” I carry nitro at a low dosage. I am now 73 but remember having these episodes back to my childhood. My mother and brother made fun of me for years because I didn’t want to play in the snow. As an adult, I moved to Arkansas where I rarely see snow. Now that I understand the causes and solutions, I seldom have a problem. My cardiologist insists on doing routine cardiac catheterizations and always has stents at the ready. He has never found a reason to insert a stent and just shakes his head. Only my latest CC found any blockage and that was in the capillaries that look like Daddy Longlegs spider legs. So I am a very lucky and probably very rare case. Note: I don’t see a repeat comment.
You didn’t mention a connection with Reynaud’s which was noted in my case. Cold, vibration and emotional stress are the stressors that bring mine on. Dressing to block cold [layered and with either ski mask or using a muffler to breath through is very effective for me. I also avoid riding on riding mowers, go carts where the vibration comes up my legs and arms are the second most frequent cause. Only once did it come from stress [I had a very low blood sugar [T1D], a full bladder and a hysterical boss yelling at me that I “was just making excuses and would NOT be allowed to leave the demo area to use the bathroom.” I carry nitro at a low dosage. I am now 73 but remember having these episodes back to my childhood. My mother and brother made fun of me for years because I didn’t want to play in the snow. As an adult, I moved to Arkansas where I rarely see snow. Now that I understand the causes and solutions, I seldom have a problem. My cardiologist insists on doing routine cardiac catheterizations and always has stents at the ready. He has never found a reason to insert a stent and just shakes his head. Only my latest CC found any blockage and that was in the capillaries that look like Daddy Longlegs spider legs. So I am a very lucky and probably very rare case.
This is so fascinating, thank you for the information! My husband has just started having these, and our son has a self limiting condition related to Reynaud’s syndrome. He ONLY has them when he is golfing, and we just couldn’t figure it out! Your comment was more helpful than you know!