Coronary Bypass Surgery, Heart Surgery, Coronary Artery Bypass Grafting (CABG)
Coronary artery bypass grafting (CABG) is used to improve blood flow to the heart in people with severe Coronary Artery Disease (CAD).
CABG is one treatment for CAD. During CABG, a healthy artery or vein from another part of the body is connected, or grafted, to the blocked coronary artery. The grafted artery or vein bypasses (that is, it goes around) the blocked portion of the coronary artery. This new passage routes oxygen-rich blood around the blockage to the heart muscle. As many as four or more major blocked coronary arteries can be bypassed during one surgery.
Overview
CABG surgery is performed to relieve angina in patients who have failed medical therapy and are not good candidates for angioplasty (PTCA). CABG surgery is ideal for patients with multiple narrowings in multiple coronary artery branches, such as is often seen in patients with diabetes.
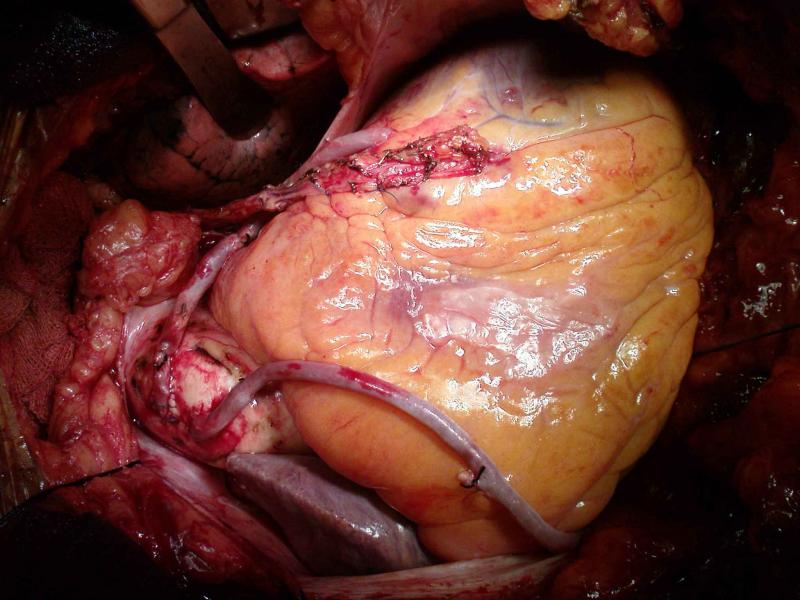
CABG surgery has been shown to improve long-term survival in patients with significant narrowing of the left main coronary artery, and in patients with significant narrowing of multiple arteries, especially in those with decreased heart muscle pump function. The most commonly used vessel for the bypass is the saphenous vein from the leg. Bypass grafting involves sewing the graft vessels to the coronary arteries beyond the narrowing or blockage. The other end of this vein is attached to the aorta. Chest wall arteries, particularly the left internal mammary artery, have been increasingly used as bypass grafts.
This artery is separated from the chest wall and usually connected to the left anterior descending artery and/or one of its major branches beyond the blockage. The major advantage of using internal mammary arteries is that they tend to remain open longer than venous grafts. Ten years after CABG surgery, only 66% of vein grafts are open compared to 90% of internal mammary arteries.
CABG surgery takes about three to four hours to complete. The aorta is clamped off for about 60 minutes and the body is supported by a heart-lung machine (cardiopulmonary bypass) for about 60-90 minutes. The use of 3 (triple), 4 (quadruple), or 5 (quintuple) bypasses are now routine. At the end of surgery, the sternum is wired together with stainless steel and the chest incision is sewn closed. Plastic tubes (chest tubes) are left in place to allow drainage of any remaining blood from the space around the heart (mediastinum).
About 5% of patients require exploration within the first 24 hours because of continued bleeding after surgery. Chest tubes are usually removed the day after surgery. The breathing tube is usually removed shortly after surgery. Patients usually get out of bed and are transferred out of intensive care the day after surgery.
Up to 25% of patients develop heart rhythm disturbances within the first three or four days after CABG surgery. These rhythm disturbances are usually temporary atrial fibrillation, and are felt to be related to surgical trauma to the heart. Most of these arrhythmias respond to standard medical therapy that can be weaned one month after surgery. The average length of stay in the hospital for CABG surgery has been reduced from as long as a week to only three to four days in most patients. Many young patients can even be discharged home after two days.
A new advance for many patients is the ability to do CABG without going on cardiopulmonary bypass (“off pump”), with the heart still beating. This significantly minimizes the occasional memory defects and other complications that may be seen after CABG, and is a significant advance.
How do patients recover after CABG surgery?
Sutures are removed from the chest prior to discharge and from the leg (if the saphenous vein is used) after 7 to 10 days. Even though smaller leg veins will take over the role of the saphenous vein, a certain degree of swelling (edema) in the affected ankle is common. Patients are advised to wear elastic support stockings during the day for the first four to six weeks after surgery and to keep their leg elevated when sitting. This swelling usually resolves after about six to eight weeks.
Healing of the breastbone takes about six weeks and is the primary limitation in recovering from CABG surgery. Patients are advised not to lift anything more than 10 pounds or perform heavy exertion during this healing period. They are also advised not to drive for the first four weeks to avoid any injury to the chest.
Patients can return to normal sexual activity as long as they minimize positions that put significant weight on the chest or upper arms. Return to work usually occurs after the six week recovery, but may be much sooner for non-strenuous employment. Exercise stress testing is routinely done four to six weeks after CABG surgery and signals the beginning of a cardiac rehabilitation program. Rehabilitation consists of a 12 week program of gradually increasing monitored exercise lasting one hour three times a week.
Patients are also counseled about the importance of lifestyle changes to lower their chance of developing further CAD. These include stopping smoking, reducing weight and dietary fat, controlling blood pressure and diabetes, and lowering blood cholesterol levels.
CABG isn’t used for everyone with CAD. Many people with CAD can be treated by other means, such as lifestyle changes, medicines, and another revascularization procedure called angioplasty.
CABG may be an option if you have severe blockages in the large coronary arteries that supply a major part of the heart muscle with blood—especially if the heart’s pumping action has already been weakened.
CABG may also be an option if you have blockages in the heart that can’t be treated with angioplasty. In these situations, CABG is considered more effective than other types of treatment.
If you are a candidate for CABG, the goals of having the surgery are to:
- Improve your quality of life and decrease angina and other symptoms of CAD
- Resume a more active lifestyle
- Improve the pumping action of the heart if it has been damaged by a heart attack
- Lower the chances of a heart attack (in some patients, such as those with diabetes)
- Improve your chance of survival
Repeat surgery may be needed if grafted arteries or veins become blocked, or if new blockages develop in arteries that weren’t blocked before. Taking medicines as prescribed and making lifestyle changes that your doctor recommends can lower the chance of a graft becoming blocked.
In people who are candidates for the surgery, the results are usually excellent, with 85 percent of people having significantly reduced symptoms, less risk for future heart attacks, and a decreased chance of dying within 10 years following the surgery.
Types of Coronary Artery Bypass Grafting
Traditional Coronary Artery Bypass Surgery
This is the most common type of coronary artery bypass grafting (CABG). It’s used when at least one major artery needs to be bypassed. During the surgery, the chest bone is opened to access the heart. Medicines are given to stop the heart, and a heart-lung machine is used to keep blood and oxygen moving throughout the body during surgery. This allows the surgeon to operate on a quiet heart. After surgery, the heart is restarted using mild electric shocks.
Off-Pump Coronary Artery Bypass Grafting
This type of CABG is similar to traditional CABG in that the chest bone is opened to access the heart. However, the heart isn’t stopped, and a heart-lung machine isn’t used. Off-pump CABG is sometimes called beating heart bypass grafting. This type of surgery may reduce complications that can occur when a heart-lung machine is used, and it may speed up recovery time after surgery.
Minimally Invasive Direct Coronary Artery Bypass Grafting
This surgery is similar to off-pump, but instead of a large incision to open the chest bone, several small incisions are made on the left side of the chest between the ribs. This type of surgery is used mainly for bypassing the vessels in front of the heart. It’s a fairly new procedure, which is performed less often than the other types. This type of surgery is not for everybody, especially if more than one or two coronary arteries need to be bypassed.
Image from: http://www.medicinenet.com/coronary_artery_bypass_graft/page4.htm