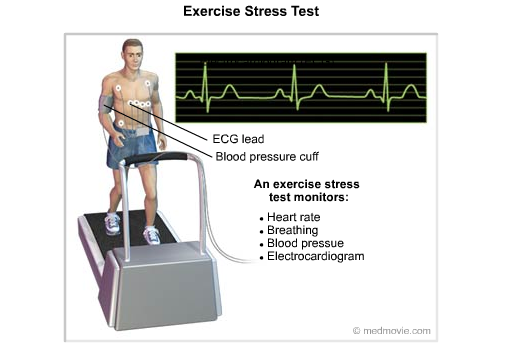
An Exercise Stress Test is a diagnostic test in which a person walks on a treadmill or pedals a stationary bicycle while hooked up to equipment that monitors the heart. The test monitors heart rate, breathing, blood pressure, electrical activity (on an electrocardiogram) and the person’s level of tiredness. It shows if the heart’s blood supply is sufficient and if the heart rhythm is normal.
In addition to the standard exercise stress test, other methods of cardiovascular stress testing include scintigraphy and echocardiography.
- Exercise stress scintigraphy uses a radioactive tracer to enhance abnormal areas of myocardial blood flow. Stress scintigraphy can be performed with pharmacologic agents instead of exercise if the patient’s condition does not allow sufficient physical activity to perform the study.
- Echocardiography has recently been used in combination with exercise or pharmacologic stress testing as yet another form of noninvasive cardiac evaluation.
Exercise stress testing provides a controlled environment for observing the effects of increases in the myocardial demand for oxygen; the presence of significant coronary artery disease results in EKG changes that can be observed and recorded.
Stress ECHOCardiogram
Dobutamine Stress Test:
Youtube videos from Cardiosmart.

Indications for the Standard Exercise Stress Test
- Patients who present with symptoms of coronary artery disease, including the classic anginal symptoms of chest pressure or pain that occurs with or without exertion. Atypical presentations or anginal equivalents, such as shortness of breath or dyspnea on exertion, are also appropriate indications for this study.
- Asymptomatic healthy persons may be considered as candidates for exercise stress testing if they are in high-risk occupations (e.g., pilots, firefighters, law enforcement officers, mass transit operators). In addition, the American College of Sports Medicine (ACSM) recommends an exercise stress test for all women 50 years of age and older and all men 40 years of age and older who plan to engage in vigorous exercise.
- An exercise stress test may also be considered in asymptomatic patients who have two or more risk factors for coronary artery disease or a concurrent chronic disease, such as diabetes, that carries a high risk of coronary disease. Patients with valvular disorders (except those with hemodynamically significant aortic stenosis) may undergo an exercise stress test to evaluate their functional capacity, the effectiveness of treatment, their symptom complex or the need for surgical intervention.
Standard Format for Reporting the Results of an Exercise Stress Test
Items included in interpretation of the results
- Basic ECG interpretation
- Symptoms reported during stress testing
- Reason for ending exercise
- Estimate of exercise capacity in METS
- Blood pressure response
- Presence and frequency of arrhythmias or ectopy
- ECG changes (type and location) observed during the test
Conclusions
- Positive
- Negative
- Equivocal
- Uninterpretable
- Goal achieved
- Maximal
- Submaximal
ECG (or EKG) = electrocardiogram; METS = metabolic equivalents.
Interpretation
An interpretation of the baseline ECG is included in the report, noting any abnormalities and changes that occurred with changes in position (standing, lying or sitting). Symptoms occurring during the exercise stress test are usually reported as well. Most commonly, these comments are described as “fatigue,” “legs tired,” “chest pain/pressure,” “shortness of breath,” etc. If these symptoms were severe, they may have been the reason for discontinuing the test. Other reasons cited for stopping the test may be “target heart rate achieved,” “exercise stopped per patient’s request,” “equipment malfunction” or “ECG findings or criteria were met.”
Also usually described are the duration of the exercise period and the workload in METS (metabolic equivalents, or resting oxygen consumption of about 3.5 mL per kg per minute). The interpreter may also add subjective comments about the patient’s exercise capacity; for example, the report may state “poor exercise tolerance (3 to 4 METS)” or “good exercise tolerance (10 to 11 METS).” The cardiorespiratory fitness levels established by the ACSM can serve as general guidelines.
Comments 1
Pingback: Recurrent Chest pain - Cardiac Health