In determining a treatment strategy for a patient with CAD, there are a variety of considerations that need to be made when selecting the appropriate treatment:
For long–term graft patency the use of the Left Internal mammary artery bypass to LAD has long proven to be vastly superior to any other intervention. In the few hospitals where Off-Pump minimally invasive CABG (MIDCAB), using LIMA to LAD[1] has been compared with LAD-PCI[2], target vessel-related recurrence of angina was significantly higher in the DES group than in the MIDCAB group.
In addition, economic analysis from the ACRE study[3] has shown that after one year CABG is more cost-effective than PCI, based on the costs of CABG or PCI (including hospital stay), drugs, admissions for chest pain, general practitioner visits, outpatient appointments, and visits to the emergency room.
In comparison with CABG, the high costs of PCI, recurrence of angina, absence of a mortality benefit, absence of a marked gain in quality of life and especially, the ongoing need for repeat procedures, have all been reported in these other trials.
Despite these considerations PCI usage has increased rapidly during the past 10-15 years, without consideration of the medical/economic consequences, or the 2012 AHA Standard of Care Recommendations that include CABG for patients with 3V CAD and L main disease, especially in diabetics and those with reduced cardiac function, in contrast to CABG where surgery volumes have decreased from 30-50% during the same period.
In 2012, Keith Fox from the Department of Cardiology, Centre for Cardiovascular Science, University of Edinburgh[4], proposed a treatment algorithm for patients with stable coronary artery disease based on symptoms, evidence of ischemia and a Fractional Flow Reserve <0.8:
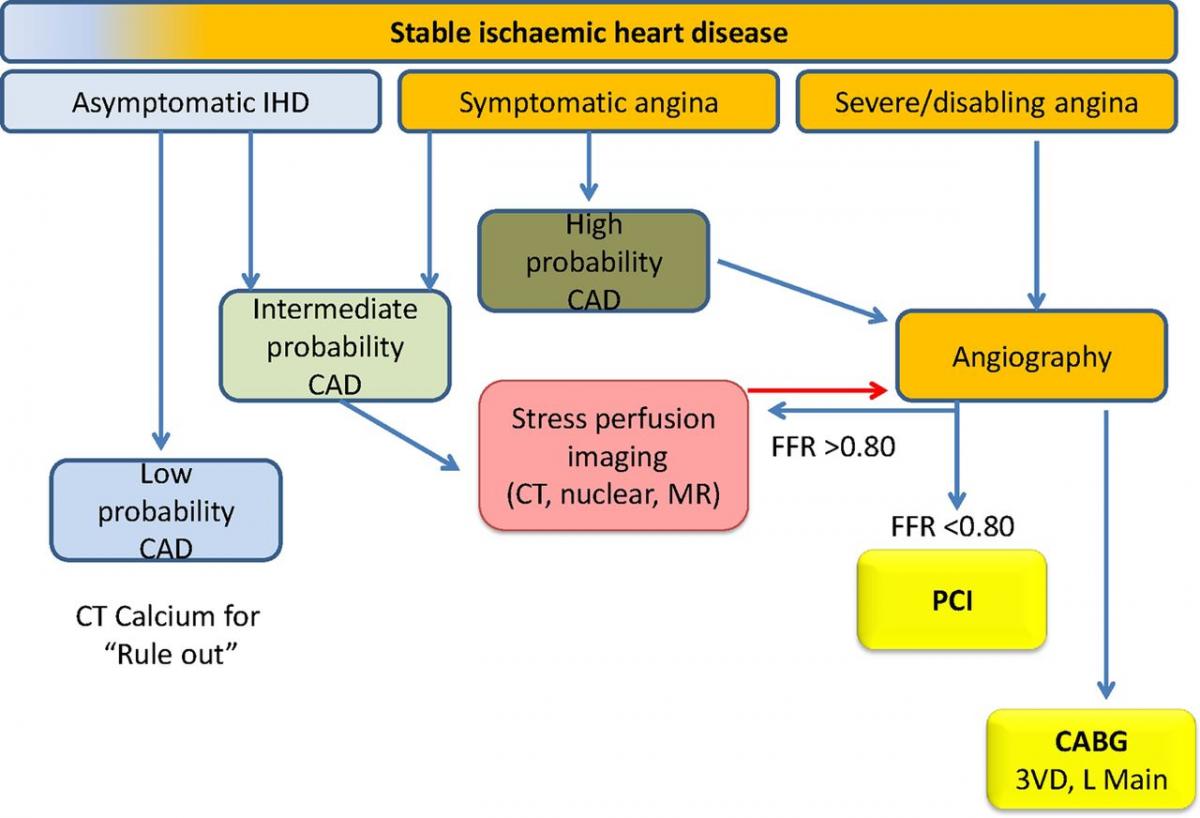
Symptom and ischaemia-guided approach to revascularisation in stable ischaemic heart disease. CABG, coronary artery bypass grafting; CAD, coronary artery disease; FFR, fractional flow reserve; PCI, percutaneous coronary intervention; 3VD, three-vessel disease.
Whether this approach is now used effectively in clinical practice is unknown.
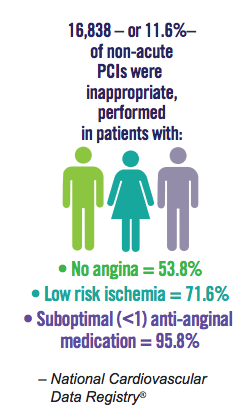
With this in mind, article in the NYTimes on [5] once again has confirmed that rational guidelines have little effect on clinical practice: “Far too often, studies show, stents continue to be implanted in patients who stand to gain little if any benefit. Last month, two of the country’s largest medical organizations identified the procedure commonly used to place a stent — called a percutaneous coronary intervention, or angioplasty — as one of five highly overused medical interventions.”
This fact was once again emphasized in the recent treatment of President Bush – not even a US president is safe from the oculo-stenotic reflex!
[1] Because of low case volumes MIDCAB is not necessarily comparable with traditional CABG with LIMA to LAD outcomes.
[2] Five-year follow-up of drug-eluting stents implantation vs. minimally invasive direct coronary artery bypass for left anterior descending artery disease: a propensity score analysis, Pierre Yves Etienne et al, European Journal of Cardio-Thoracic Surgery (2013) 1–7 doi:10.1093/ejcts/ezt137
[3] Cost effectiveness of clinically appropriate decisions on alternative treatments for angina pectoris: prospective observational study, S C Griffin et al.; BMJ, doi:10.1136/bmj.39129.442164.55
[4] COURAGE or FAME…? Who should have percutaneous coronary intervention in stable coronary artery disease? Heart 2013;99:442–444.
[5] Heart Stents Still Overused, Experts Say, NYTimes, August 15, 2013
Comments 1
Pingback: Effect of PCI on Long-Term Survival in Patients with Stable Ischemic Heart Disease | Cardiac Health