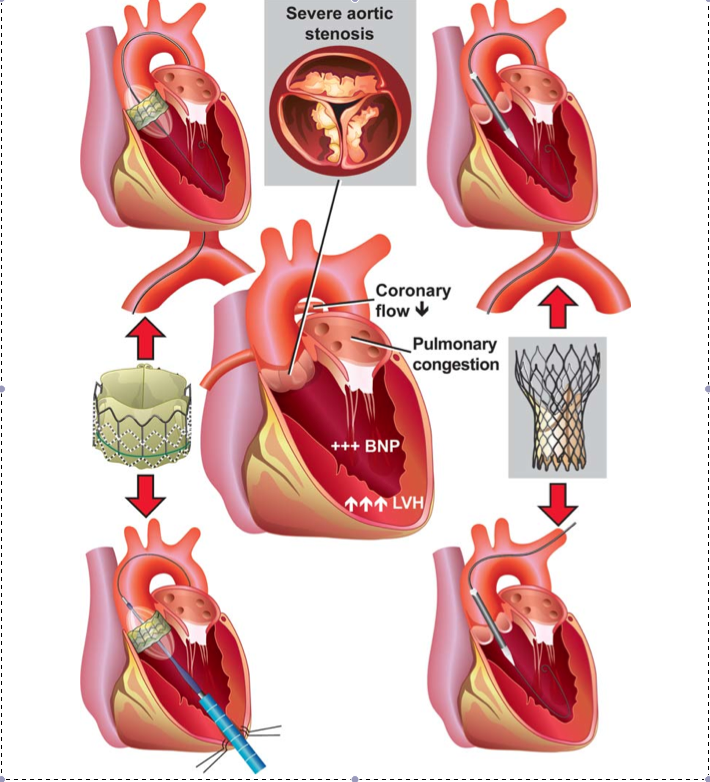
There are many patients with severe aortic stenosis and coexisting conditions who are not candidates for surgical replacement of the aortic valve. For those patients trans-catheter aortic-valve implantation (TAVI) may be an option.
Once severe aortic stenosis is diagnosed, a less than 50% survival rate in the first 2 years after symptoms appear is projected. Traditional Aortic valve replacement can be performed at very low risks in otherwise healthy patients and offers excellent survival. However, in clinical practice, at least 30% of patients with severe symptomatic aortic stenosis do not undergo surgery for replacement of the aortic valve, owing to advanced age, left ventricular dysfunction, or the presence of multiple coexisting conditions. In those patients, TAVI may offer an alternative.
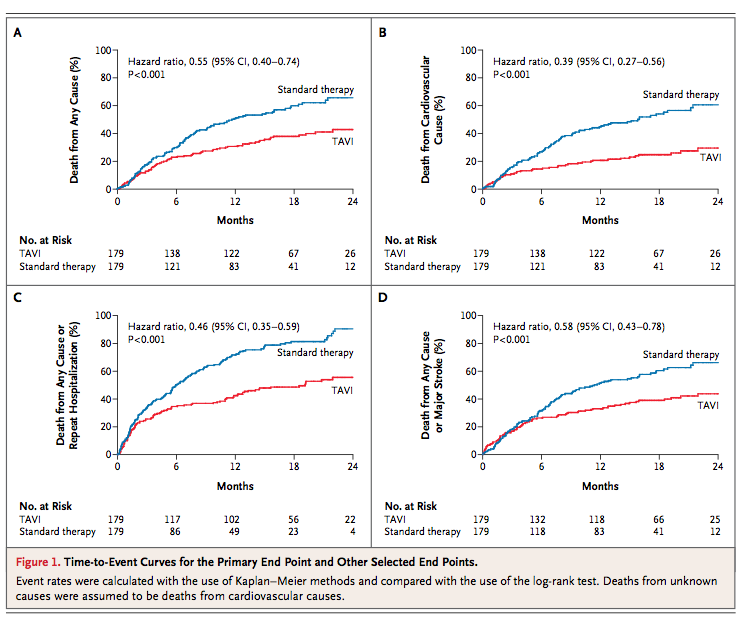
A number of studies in the US and Europe have recently been published, showing acceptable early results in this very sick sub-group of patients with severe aortic stenosis.The PARTNER trial compared TAVI with standard therapy, including aortic balloon angioplasty. It should be noted this comparison suffers from the fact that outcomes with medical management in these type of patients are uniformly poor. Survivors had a significantly lower rate of death at 1 year, fewer hospital readmissions, and a reduction in cardiac symptoms (lower New York Heart Association functional class). These improved outcomes were achieved at the cost of a significant increase in the rate of major strokes and vascular events. However, the initial 5% procedural mortality and stroke rate in the TAVI group was compensated for at one year:
Other studies have reported mortality rates ranging from 4.4-22%, stroke 0-12%, and a need for pacemaker implantation of 12-39%. Likewise, TAVI was associated with significant para-valvular leak rate as compared to a standard procedure.
Paraphrasing an editorial in the same NEJM issue, “… TAVI needs to be measured against the “yardstick” of traditional Aortic valve replacement, which can be performed safely in a large group of patients, including the very elderly and which remains the standard for the treatment of aortic stenosis. TAVI should be reserved for patients at inordinately high risk who are not suitable candidates for surgery and who have decreased life expectancy…”
I concur with this editorial, and would add a fear that TAVI will soon be part of the standard procedures of invasive cardiology, used on a much less selected group of patients and that inferior outcomes will be explained away with arrays of studies, not unlike those involving PCI vs. CABG.
Dr T
References:
1): Transcatheter Aortic-Valve Implantation for Aortic Stenosis in Patients Who Cannot Undergo Surgery, Leon, MB, Smith CR, et al, N Engl J Med 2010; 363:1597-1607
2): Transcatheter Aortic Valves — Where Do We Go from Here? Harold L. Lazar, M.D. N Engl J Med 2010; 363: 1667-68.
3): One year follow-up of the multi-centre European PARTNER transcatheter heart valve study, PARTNER EU, Thierry Lefevre et al. European Heart Journal (2011) 32, 148–157)